The above image is from the Textbook of Anatomy and Physiology, by Kimber, Gray, and Stackpole. Published by The Macmillan Company; eleventh edition, 1944. (Image courtesy of Laurel Leaf Farm.)
This post, part of a series on the disaster of COVID-19 and the COVID-19 “vaccines”, is dedicated to the memory of Yours Truly’s cousin Bill, who “died suddenly and unexpectedly” in September 2023. Today’s offering will speak to what might be called a “tangential” issue: the American Medical Association (the AMA.) Yours Truly will make it clear at the outset that today’s post is not to be construed as a “hit piece” on the AMA; also, that there are likely many members of the AMA who are not “beholden” to blindly accept everything that the AMA publishes. The point of today’s piece, in one’s opinion, is that the current AMA apparently sees itself as a sort of “arm” of “establishment medicine” (in other words, of the FDA and the CDC); in addition to becoming an organization that advocates what may be called “medico-political” viewpoints. First, before discussing the AMA Edhub, some items about the organization:
It is fair to posit that the American Medical Association (also referred to as the AMA) is the largest and most powerful medical doctor organization in the United States. The AMA has also become, arguably, the most powerful medical organization lobbyist in the United States House of Representatives and the United States Senate.
The American Medical Association was founded in 1847. In the year 2022, it had 271,660 members, and $493,147,829 in revenue (per Wikipedia: https://en.wikipedia.org/wiki/American_Medical_Association). Further information on the history of the organization is found here: www.ama-assn.org/about/ama-history. The AMA does not publish a membership directory as of the year 2021: https://myama.my.site.com/s/article/Does-the-AMA-have-a-member-directory, stating the following: “The privacy of our customers’ [presumably, this means “members'”] data is something we take very seriously.” On the other hand, the 2022 census of the Federation of State Medical Boards listed a total of 1,044,734 licensed physicians in the United States (www.fsmb.org/advocacy/news-releases/fsmb-physician-census-identifies—1044734-licensed-physicians-in-u.s/). This means that 26% (271,660) of the licensed physicians in the United States belong to the AMA. (Side note: members of the AMA have “exclusive discounts” towards purchasing new Mercedes-Benz and Volvo cars: www.ama-assn.org/member-benefits/personal-member-benefits-discounts/auto-transportation-discounts).
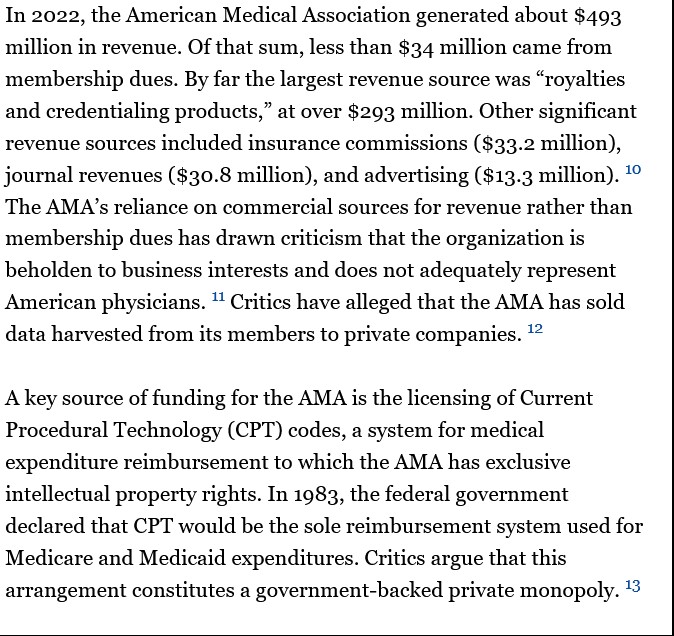
The American Medical Association is a “heavy-spender” lobbyist to the United States federal government, spending at least $15 million per year in this effort since 1998: www.influencewatch.org/non-profit/american-medical-association/ (this article also has a history of the AMA, the organization’s views on healthcare policies, and so forth); in the year 2022 alone, the AMA spent $21,060,000 on federal government lobbying, per Open Secrets: www.opensecrets.org. A screenshot of the Influence Watch report on the AMA is below. Note that the AMA owns the exclusive rights to the medical expenditure reimbursement codes system for Medicare and Medicaid (the CPT codes.) This entails the payments of “rights and royalties” to the AMA. For further information, please refer to: https://microwize.com/why-do-i-have-to-pay-a-fee-to-use-cpt-code/, 14 December 2022.
The AMA, as can be inferred from the above screenshot, is also involved with the FDA and the CDC. Two examples: the AMA’s lobbying efforts with these agencies regarding advocacy for COVID-19 programs of various types, along with other advocacy efforts: www.ama-assn.org/delivering-care/public-health/covid-19-amas-recent-and-ongoing-advocacy-efforts (1 June 2022 report); www.ama-assn.org/topics/coronavirus-vaccines; and, www.ama-assn.org/delivering-care/public-health/covid-19-2019-novel-coronavirus-resource-center-physicians (updated 17 April 2024.)
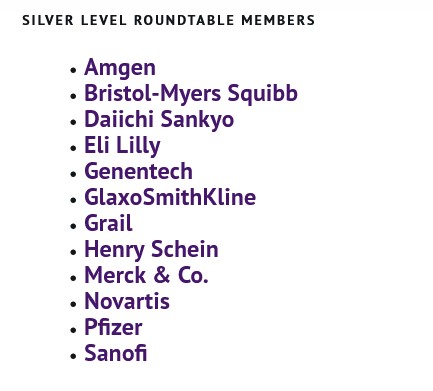
The AMA has a “membership dues schedule”, ranging from $20 for a 1-year medical student membership, through a $420 per year dues fee for a “Regular practice” physician who belongs to the AMA. And, there are other types of membership available (corporate and e-membership.) www.amanet.org/membership/. There are other types of corporate and institutional memberships available through the AMA Foundation, also called the “Roundtable.” (https://amafoundation.org/donors/corporate-donors/). A screenshot of the “Silver Level” corporate donor list to the AMA is below (the “Silver Level” requires a $30,000 contribution to the AMA Foundation, presumably paid each year by each donor company):
Two other areas of AMA effort are in physician Continuing Education and in publishing. Members of the AMA who are licensed medical doctors can fulfill their Continuing Education accreditation through courses offered by the organization. These courses are offered via various methods: www.ama-assn.org/topics/contuning-medical-education. The AMA also publishes a journal, known as JAMA (Journal of the American Medical Association): https://jamanetwork.com/. The website is open-access, and there are hundreds of peer-reviewed articles from thirteen different JAMA specialty journals available for public reading for several months after articles are published. As might be expected, the AMA advocates for what might be called “establishment medicine” — for example, championing FDA-authorized or FDA-approved treatments and drugs for COVID-19 infection.
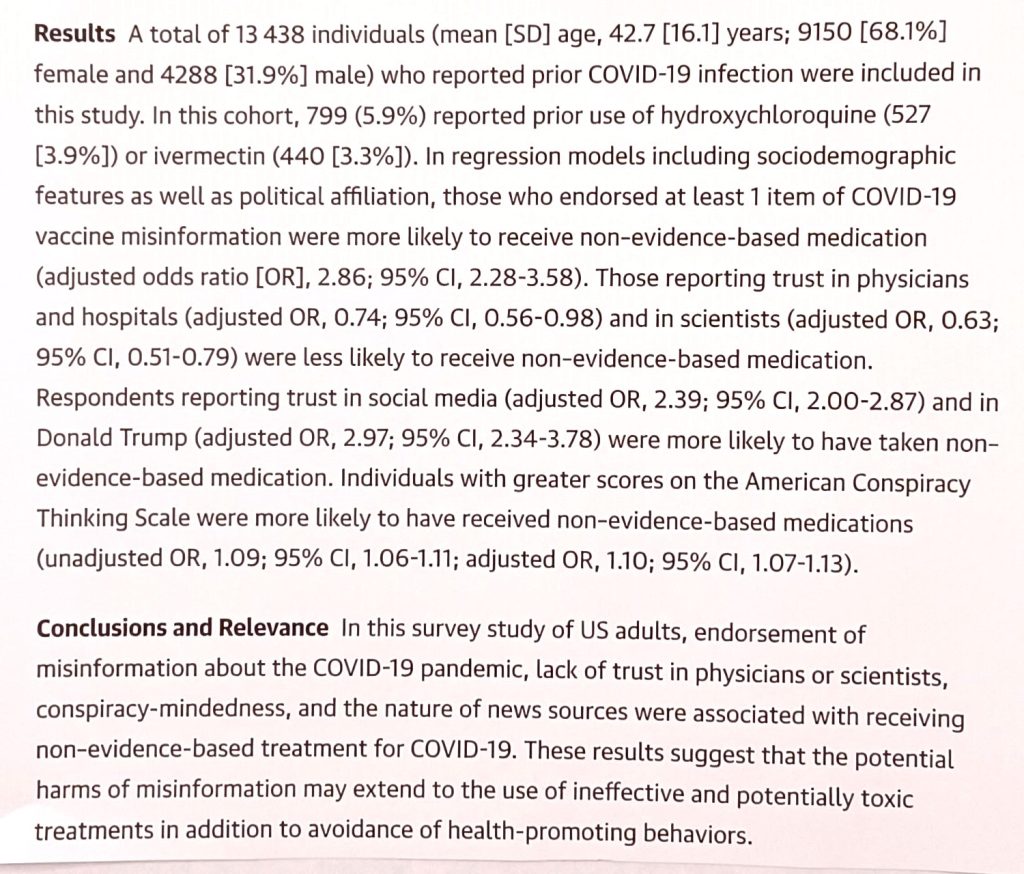
Yours Truly will include part of the Abstract (below) of a recent paper published in JAMA, regarding people who mistrust “establishment medicine” (in other words, they may mistrust FDA-authorized or FDA-approved) treatments for COVID-19. This paper, in Yours Truly’s opinion, demonstrates the AMA’s official attitude towards those who question or refuse “establishment medicine” treatment of COVID1-19 and pursue other, alternative treatments — that these people are “being misled” by “misinformation” and may use that “misinformation” to avoid “health-promoting behaviors.” The paper is found here: https://jamanetwork.com/journals/jama-health-forum/fullarticle/2809985, “Misinformation, Trust, and Use of Ivermectin and Hydroxychloroquine for COVID-19”, Roy H. Perlis, MD, et al., published 29 September 2023. Dr. Perlis is Associate Editor of JAMA Network Open.
It appears that the AMA is “leading the charge” on “medico-political” topics, such as “climate change”, DEI (Diversity, Equity, and Inclusion), “equity of access to care” for illegal immigrants, “gender equity”, and more.
This leads to the AMA EdHub discussion.
The AMA EdHub website features online courses and Continuing Education (CME) fulfillment modules for physician members (https://edhub.ama-assn.org). These courses and modules are presented in various ways: webinars; video and/or audio courses; papers to be read; and so on. One does not have to be a member of the AMA in order to access and read many of the courses and modules; in fact, the AMA states that, “The AMA EdHub is open to anyone.” (https://education.ama-assn.org/help/, the “FAQ’s” section); interested persons simply open an account. However, only licensed physicians who belong to the AMA can fulfill their CME credits using the AMA EdHub. https:///edhub.ama-assn.org/pages/ama-cme, section “Target Audience“; and, www.ama-assn.org/member-benefits/personal-member-benefits-discounts/ama-ed-hub-member-benefits.
On other hand, the AMA EdHub provides a good “snapshot” of the current modes of thought in “establishment medicine”, as well as current trends in treatment and in the teaching of medical school students, among other topics. For example, there are CME modules and online courses related to DEI; to “anti-racism in medicine”; “equitable patient care”; and other what may be termed “medico-political” topics areas. Here is a link to one such example, a CME module: https://edhub.ama-assn.org/clinical-problem-solvers-antiracism-podcast/audio-player/18843339, “Episode 23 – Anti-Blackness, Anti-Fatness, and Food Shaming”, 9 January 2024. This somewhat over one hour audio module (with a Transcript that can be read) can be used, after the physician takes the Quiz, to earn one CME credit. The Learning Objectives listed for this module are: “1. Explain how anti-fatness and food shaming culture in the US is rooted in anti-Blackness 2. Describe the intersection of policing and the court systems with anti-fatness and food shaming 3. Identify ways to navigate clinical interactions with patients while respecting them and affirming their experiences with food and fatness.”
The AMA Edhub also has a department devoted to “health equity” — https://edhub.ama-assn.org/ama-center-health-equity. From the main page of the link: “Education from AMA Center for Health Equity AMA’s online education to empower individuals ad organizations, in healthcare and beyond, in advancing racial justice and equity.”
It appears that one area of particular emphasis in the AMA Center for Health Equity has to do with “gun violence prevention” — through “education” of medical students, practicing physicians, and patients — and working with the United States Congress. Here is a link to a recent video CME fulfillment presentation from the AMA Center for Health Equity: https://edhub.ama-assn.org/ama-center-health-equity/video-player/18867531, “Prioritizing Equity: Embracing Public Safety and Health for Improved Firearms Violence Prevention“, 2 April 2024. This video presentation has a Transcript that can be read. It appears, from reading the Transcript, that the AMA’s position on “gun violence prevention” goes beyond working through the criminal justice system. According to Dr. Megan Ranney, MD, one of the speakers interviewed on the video, “…it’s about separating someone from the potential to access a firearm at that moment of desperation, anger, impulsivity, hopelessness.” Dr. Ranney also states that, “…the amount of violence that youth are exposed to in urban neighborhoods far outstrips the amount of violence that people are exposed to in the military.” (Italics added)
The AMA EdHub has other areas of interest that offer online CME courses for AMA physician members, among them: promoting “race-conscious” admissions to higher education, including to medical schools: and, courses from The Fenway Institute, an organization that advocates for LGBTQIA+ and Transgender issues and persons. Here are links to examples of these AMA EdHub areas of interest: https://edhub.ama-assn.org/ama-center-health-equity/audio-player/18868328, 2 April 2024; “The SCOTUS Affirmative Action Ruling The Cost to the Physician Workforce and Historically Minoritized Communities (with a Transcript that can be read); and, https://edhub.ama-assn.org/fenway-institute-edu/video-player/18638799, 2 September 2021, “Affirming Care for People with Intersex Traits.”
In Yours Truly’s opinion, understanding the AMA EdHub is an important part in understanding how the AMA works to influence healthcare treatment practices, healthcare policies; and the United States Congress, through the AMA’s lobbying efforts.
Peace, Good Energy, Respect: PAVACA




































Certianly not the AMA we heard about growing up and explains why the Dr’s Office keeps asking for my pronouns on it’s medical forms, though they don’t dare do it in person.
This will definitely come in handy when dealing with the parts of the corrupt woke medical establishment that take themselves seriously 
para59r
Thank you, you are very kind.
It is disconcerting, to say the least, to read what Dr. Megan Ranney states in today’s post about how urban youth in America face violence that “far outstrips” the violence that is dealt with by American military personnel.
Leave the pronoun stuff blank. Make them ask if they really believe it is important. .
Thank you, PAVACA – for yet another outpouring of vital information!
AMA has been corrupted by power and money. They are now part of the world health machine pushing deadly protocols for big pharma against patients’ best interest. No doubt big pharma pays very well for this service.
GA/FL
Thank you so much.
Big Pharma does pay “very well” to be part of the “world health machine” that pushes the dangerous and deadly COVID-19 “vaccines”, mRNA-based “vaccine” development, and so on.
For example, the “Gold Level” required donor amount from corporations (including Big Pharma corporations) to the AMA Foundation Roundtable is $50,000.
It’s not the American Medical ASSociation for nothing – aka A$$ociation.
The AMA links right back to J.D. Rockefeller and EUGENICS!
The Rockefellers, The Flexner Report, The AMA, and their Effect on Alternative Nutritional (botanical) Medicine
Gail Combs
Thank you so much for this. Why am I not surprised?
Yours Truly will call attention to the screenshot from the Perlis paper cited in today’s post, regarding the paper’s mention of the American Conspiracy Thinking Scale. This is not a detail to be overlooked — as it ties into the “medico-political” viewpoints of the AMA, as regards influencing patient care, “anti-racism”, the LGBTQIA+ “agenda”, and other aspects of human interaction.
The American Conspiracy Thinking Scale (ACTS) is a contrived “scale” that “measures” the “extent” of thinking about, and/or belief in, certain “conspiracy theories.” The “science” of studying how the American people think about “conspiracy theories” is relatively new.
A paper that uses the ACTS concept to “label” the “extent” that Americans (in particular, Republicans) think about, and/or believe in, certain “conspiracy theories”, is detailed here:
https://doi.org/10.1038/s41598-022-25617-0
“The psychological and political correlates of conspiracy theory beliefs”
Uscinski, J., et al.
published 15 December 2022
Yours Truly: This paper attempts to “prove” that certain “conspiracy theories” are believed by Americans, and Republicans in particular.
The “study” for the paper was funded by grants from the National Science Foundation.
The National Science Foundation (NSF) is an agency of the United States federal government, and as such, receives government grants for research.
The National Science Foundation collaborates with another federal agency, the National Institutes of Health (NIH.)
From the Introduction to the “paper”:
“Going further, should we expect because, for example, narcissism is associated with Holocaust denial and support for violence with QAnon beliefs that, on average, those exhibiting a tendency toward generalized conspiracy thinking are also likely to be narcissistic or supportive of violence?” (bolding mine)
Here is a screenshot of one of the figures in the “paper.” The white-banded areas on the figure relate to how “partisans” (Republicans or conservatives) think about certain “conspiracy theories.” According to the authors, it appears that “partisan” thinking about these “conspiracy theories” is high.
https://new.nsf.gov/about
https://new.nsf.gov/sbe/updates/nsf-nih-science-of-biomedical-science
“Joint research program between National Science Foundation and the National Institutes of Health to broaden participation in the science of biomedical science”
24 February 2024
Thank you for your efforts to make sense of so much bullshit!
barkerjim
Thank you, you are very kind.
“non-evidence based medication” sounds like NewSpeak from 1984, when taken in the context of contempt for HCQ &/or IVM as regards to effective treatment &/or prevention of Covid 19. That example of Peter Navarro’s confrontation w/ Dr. Fauci, having more than 50 studies showing the effectiveness of HCQ to refute the lies, comes to mind here.
Thank you for this detailed presentation PAVACA. I hope to peruse some of the JAMA articles of interest when time permits. When my son Josiah was in the NICU (before heart surgery) at his birth hospital I did A Lot of research on his various then known conditions at the hospital library, having access via my mom’s employment there. It was informing, but also pretty overwhelming then, so I take such knowledge forays now w/ a grain of salt & when I have the mental & emotional energy to dive in a bit deeper into the sludge…
Valerie Curren
Thank you, you are very kind.
This concept of “non-evidence based medication” was the “rationale” for the EUA that the FDA gave for the “2023-2024 Formula COVID-19 Vaccines” made by Pfizer-BioNTech and by Moderna. These “vaccines” had only been tested on a very small group of lab mice (all of whom died), NOT EVER on humans. But the FDA issued the EUA anyway — based on the “safety and efficacy” of the PREVIOUS “COVID-19 booster shots” formulations by these companies.
Given this “track record”, it is fair to assume that whatever “newest COVID-19 booster shot vaccine” is given an EUA for use in the fall of this year (that would make this “newest” product the “2024-2025 Formula COVID-19 Vaccine”) will be following a similar “rationale.”
Regarding reading papers — it can be a tough slog. It seems that the English language sometimes gets “lost in the shuffle.”
It’s like the EUA has replaced due diligence AND safety testing like how “continuing resolution” has replaced “budget”…sigh…